Many families assume that more providers, more hours, and more services mean better support. The reality is often the opposite. A large, uncoordinated team can produce contradictory advice, competing priorities, and a child who gets lost between settings.
This guide covers how to build a support team that is focused, aligned, and accountable — and how to manage the team over time so it continues to serve your child’s actual needs.
What a good team actually does
A good support team does not just provide services. It aligns around shared priorities so that the child experiences consistent support across home, school, and clinic.
This sounds obvious, but it rarely happens naturally. Without intentional coordination, each provider works on their own goals using their own methods with their own definitions of progress. The child adapts to each setting differently, skills do not transfer, and the family becomes the translator and coordinator between worlds that should be connected.
The core functions of a good team:
- Shared priorities. Everyone agrees on the top 3-5 goals that matter most right now.
- Clear roles. Each person knows what they are responsible for and how it connects to the shared priorities.
- Consistent communication. Regular updates — even brief ones — keep everyone informed without requiring marathon meetings.
- Unified approach. The strategies used at home, school, and therapy should be compatible. If the ABA therapist is teaching requesting with picture cards while the speech therapist insists on verbal-only, the child is caught between two systems.
- Accountability. Progress is tracked, goals are reviewed, and approaches are adjusted when things are not working.
Who should be on the team
The core team should be small — typically 3-4 people who are directly involved in the child’s daily life and can make decisions quickly.
Core team:
- You (the parent). You are the only person who sees the child across all settings. You are the continuity. Your observations are data.
- Primary therapist or BCBA. The person who designs and supervises the therapy program.
- Classroom teacher or school contact. The person who sees the child in a group learning environment daily.
Extended team (as needed):
- Speech-language pathologist. Especially important when communication is a primary target.
- Occupational therapist. When sensory or motor skills are significant barriers.
- Developmental pediatrician. For medical management, medication decisions, diagnostic updates.
- Other specialists. Added only when a specific need cannot be met by the core team.
The key principle is: add people only when there is a specific need they uniquely address. Every additional team member adds coordination cost.
Aligning around shared priorities
The most effective alignment tool is also the simplest: a one-page plan.
The one-page plan contains:
- The child’s name and current date
- The top 3-5 priorities for the next month (not 15 goals — three to five)
- For each priority: who is responsible, what the approach is, and how progress is measured
- Communication protocol: how updates are shared, how often, and by whom
This document is not a legal instrument like an IEP. It is a coordination tool. Print it. Share it with every team member. Tape it to the refrigerator. Bring it to meetings. Update it monthly.
When everyone is looking at the same short list of priorities, several problems resolve themselves:
- Providers stop working on contradictory goals
- Parents stop feeling like they need to keep track of 12 different plans
- The child experiences more consistency across settings
- Progress becomes easier to evaluate because everyone is measuring the same things
Judging team quality
A team that meets regularly but never changes anything is a team that is going through the motions. Quality shows up in action, not in meeting frequency.
Signs the team is working:
- Goals are being reviewed and updated (not sitting unchanged for months)
- Different providers reference each other’s work (“Speech told us requesting is up, so we’re adding more complex choices in ABA”)
- The child is making visible progress in daily life, not just in session data
- You as the parent feel more confident and less confused over time
- Meetings produce specific action items, not just status updates
Signs the team is drifting:
- You are hearing contradictory advice from different providers
- Goals have not changed in 6+ months despite limited progress
- Meetings are update-only — no decisions, no adjustments
- The child behaves very differently in different settings (not because of context differences, but because of inconsistent approaches)
- You feel like the only person trying to connect the dots
When you notice drift, the solution is usually not a bigger meeting but a smaller, more focused conversation with the core team about what the actual priorities are right now.
Managing provider disagreements
Disagreement between providers is not a failure. It is inevitable when multiple professionals with different training and perspectives are involved in the same child’s care.
The productive way to handle disagreement:
- Ask each provider to explain their rationale. Not just what they recommend, but why. What evidence or clinical reasoning supports their position?
- Identify the shared goal. Often, providers agree on the destination (“the child needs functional communication”) but disagree on the path (“AAC first” vs. “verbal trials first”). When you identify the shared goal, the disagreement becomes about method, which is easier to resolve.
- Use daily life as the tiebreaker. Which approach is more likely to produce results that transfer to home, school, and community? Which approach can the family actually implement? Which approach fits the child’s current profile?
- Make a decision and commit. Trying both approaches simultaneously often produces confusion. Choose one, implement it consistently, evaluate after a defined period, and adjust if needed.
As the parent, you are not expected to adjudicate clinical debates. But you are the person with the broadest view of your child’s life, and that perspective is valuable in resolving disagreements that pure clinical reasoning cannot settle.
For specific questions to ask when evaluating whether a provider is delivering quality, read How to Build a Good Autism Support Team.
How the handbook organizes team decisions
Chapters 4 and 22 of the Autism Skills Handbook provide a complete framework for team building and service evaluation. Chapter 4 covers the early stages — assembling the right people, defining roles, and creating alignment. Chapter 22 covers the long game — evaluating service quality, knowing when to adjust, and making decisions that serve the child’s trajectory rather than any single provider’s preferences.
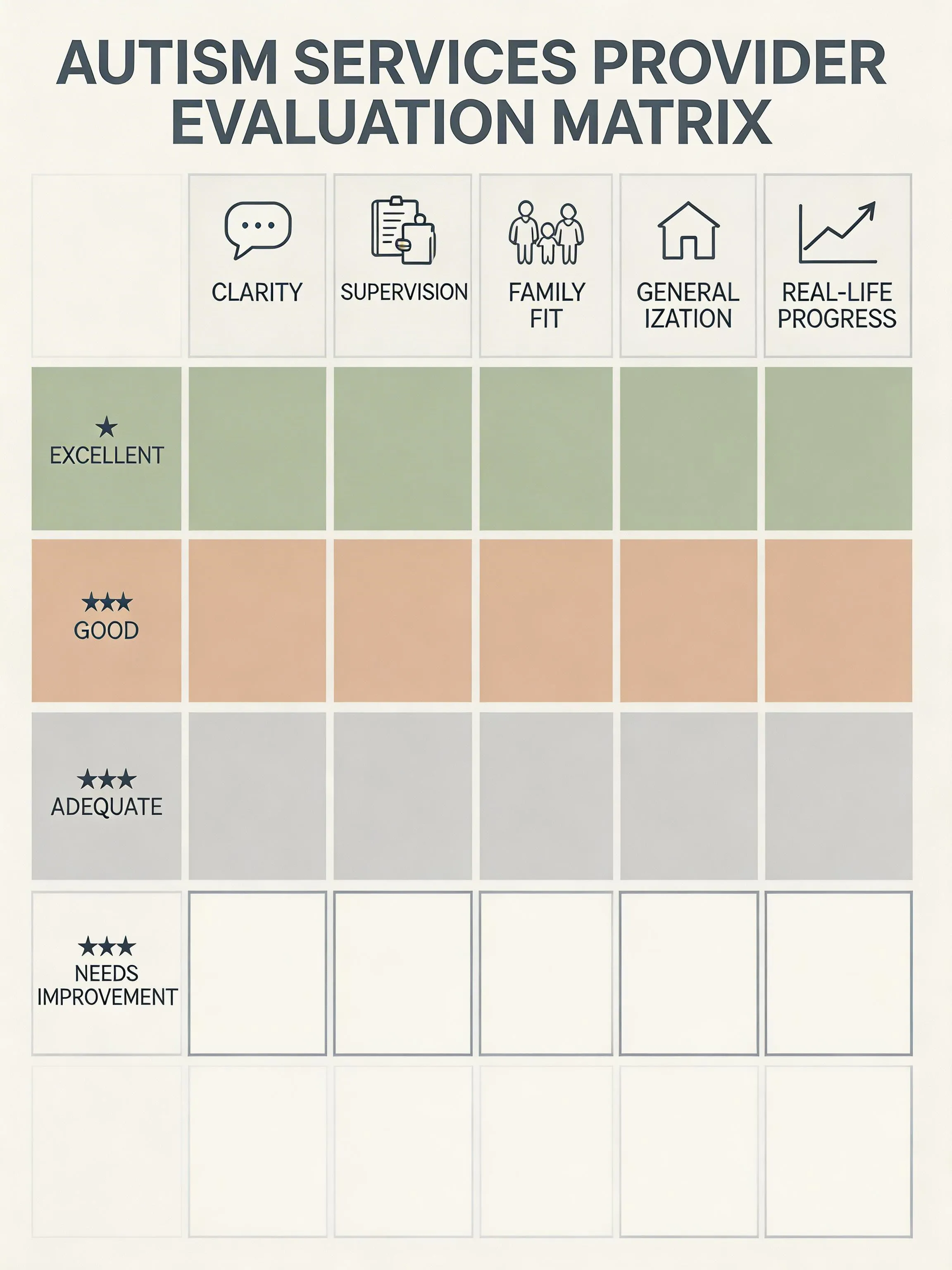
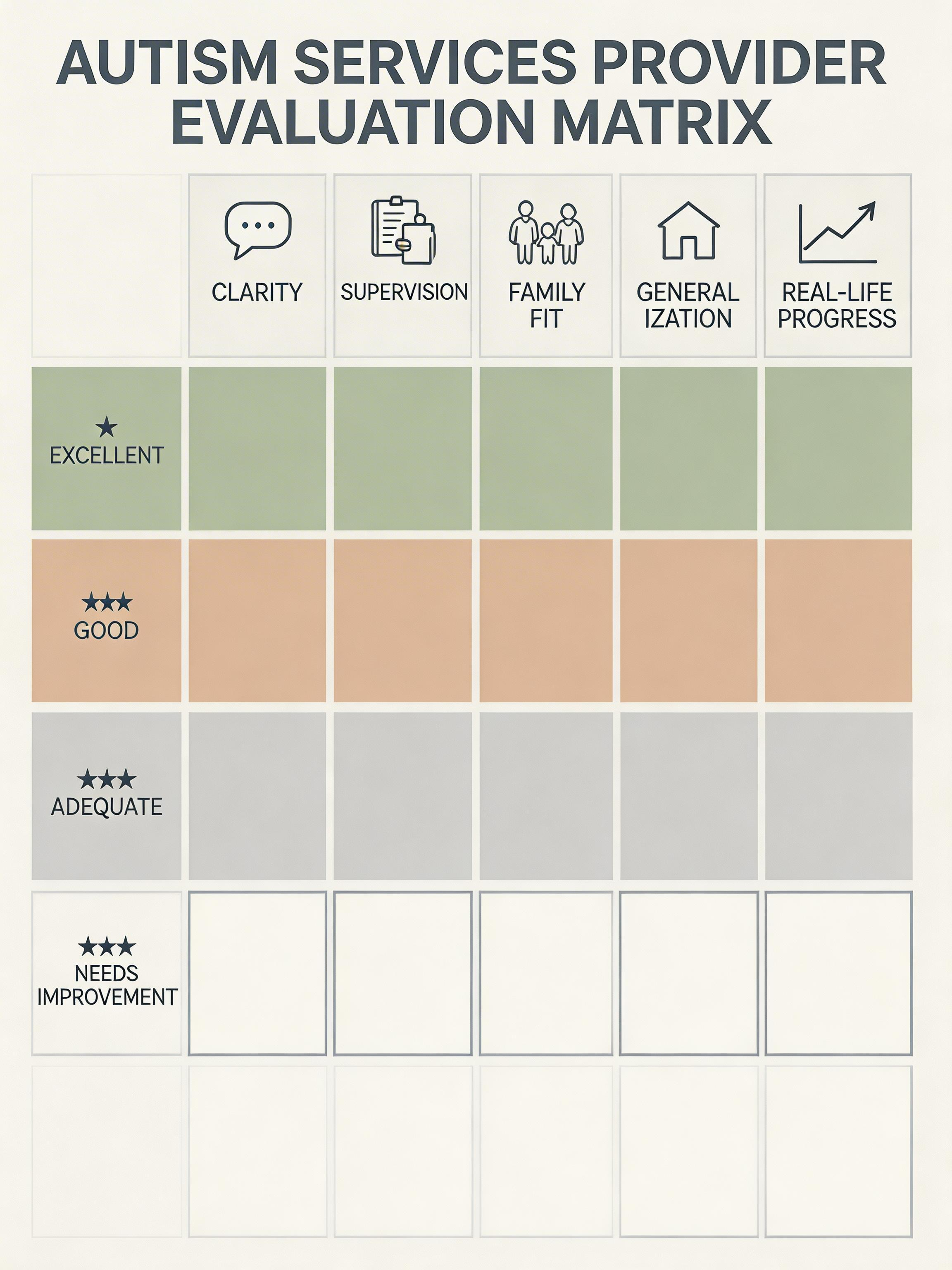
The Service Quality Review Matrix gives you a structured evaluation tool for assessing any provider against the criteria that matter most. The Team Alignment One-Page Plan template is the coordination document described in this guide — print it, fill it in with your core team, and use it as your shared reference point.
{kind=link}